Cognition and Dementia Updates
This article discusses new relevant data from 2023 and 2024 on cognition and dementia

The Book - Kindle Version Now Available Worldwide
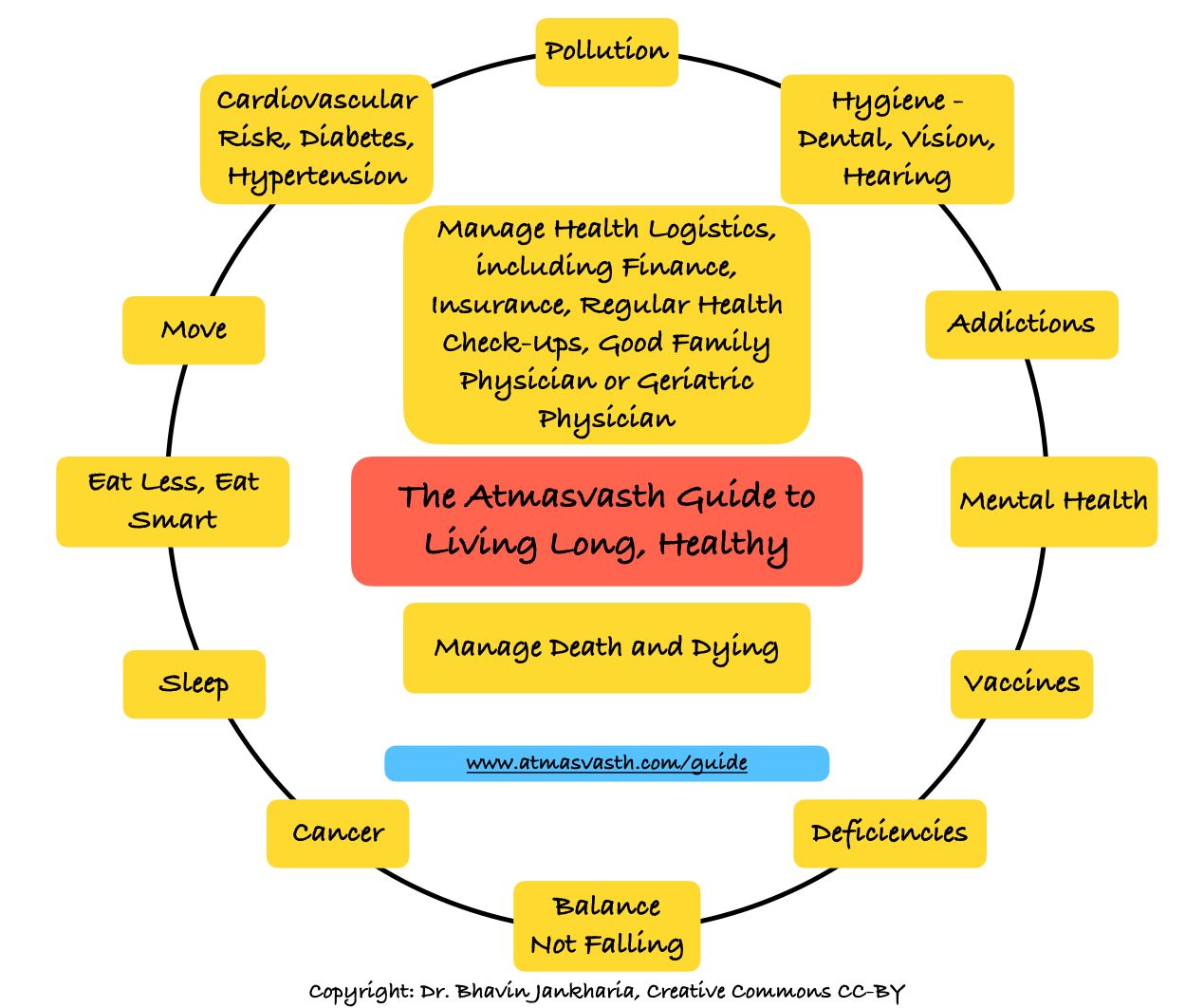
The Detailed 15-Point Guide to Live Long, Healthy
Audio
Text
Last week, I addressed the following cognition and dementia related issues in a piece titled “The Healthspan of the Mind: Preventing Cognitive Decline”.
1 Can we prevent cognitive decline?
2 Can we arrest cognitive decline or reduce its rate of decline, once it occurs?
3 What about loneliness and social isolation?
4 Should we test for cognitive decline?
The answers were based on the articles I’ve written on the subject since Dec 2020, when I started the atmasvasth project.
Dementia can be caused by various factors like Alzheimer’s (AD), vascular issues (strokes and other blood vessel problems), and other uncommon types. Therefore, there is no “one-size-fits-all” or “magic bullet” treatment or preventive method for dementia or minim al cognitive impairment (MCI).
For decades, there were limited options for individuals with MCI or full-blown dementia, except to improve their quality of life and prevent harm. However, as the world ages and dementia cases rise, there is increased interest and research. While I have mainly written about lifestyle and related factors (sensible eating, physical activity, adequate sleep, not smoking, and good social connections), it may be possible in the future to prevent and treat MCI and AD with drugs or vaccines.
This article is an update of new data and research published in 2023 and 2024.
Question 1: Can we diagnose increased risk of minimal cognitive impairment (MCI) or dementia before it is clinically apparent?
a. Genetic testing: There is good evidence now that “relative to the most common APOEε3/ε3 genotype (reference group), possessing one APOEε4 allele increases the risk of developing Alzheimer’s disease by approximately 3.7 times and being homozygous for the APOEε4 allele increases the risk up to 12 times, whereas carrying a single APOEε2 allele reduces the risk by approximately 40%, and being homozygous for APOEε2 reduces the risk even further. Besides Alzheimer’s disease risk, the APOE genotype mainly affects the age of onset of cognitive impairment, with APOEε4 carriers having an earlier age of onset and APOEε2 carriers a later age of onset than APOEε3 homozygotes.” [1] There is also “a robust association between APOEε4 and all-cause and cardiovascular mortality but not cancer mortality.” [2]
b. Blood tests: p-Tau protein blood-based assays help identify AD risk and track longitudinal status [3], and will be available in India soon.
c. Others: Physical and behavioral changes like gait disturbances [4] or making poor financial decisions may indicate dementia risk [5], though these changes are usually noticed by friends and family rather than the person themselves.
Does knowing your genetic or p-Tau risk help at this stage? Perhaps not, since there isn’t much you can do if you are homozygous APOEε4 or p-Tau positive, except lifestyle and risk modification. Maybe with more treatment options in the future, that may change.
Question 2: How can we reduce our risk of MCI or AD, or slow progression if we have MCI or AD?
I’ve already discussed lifestyle factors earlier (sensible eating, physical activity, adequate sleep, not smoking, and good social connections). Here is more recent data.
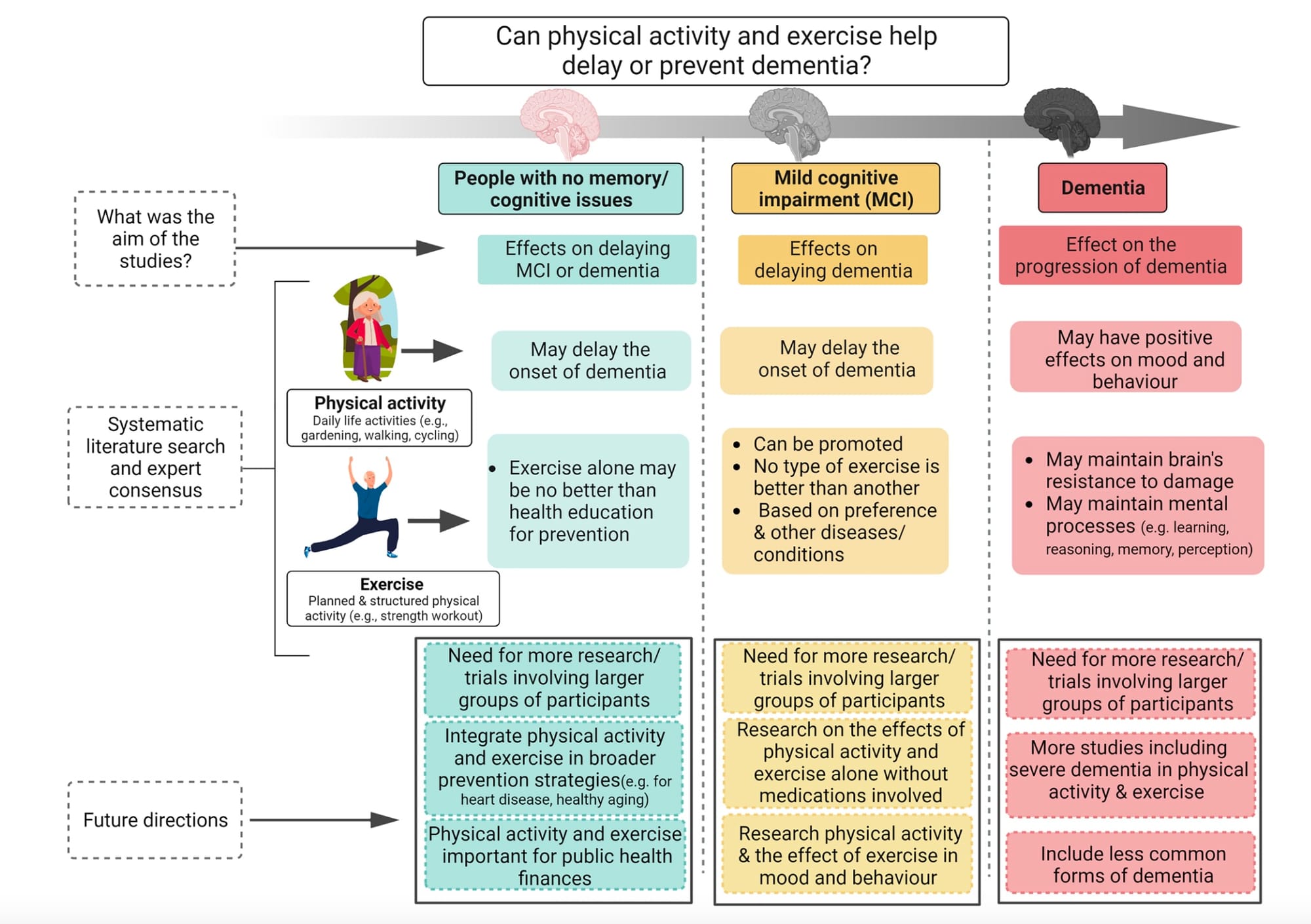
a. Physical activity: A consensus agreement [6] promotes physical activity to reduce the risk of cognitive impairment and delay its progress. Although the data on the benefits of physical activity are not perfect, the advantages outweigh any possible risk and should be promoted aggressively as this diagram shows.
b. Cardiometabolic conditions: The greater the number of cardiometabolic conditions (type 2 diabetes, heart disease, stroke) and greater the number of poor lifestyle factors (excessive alcohol consumption, excessive physical inactivity) [7], the greater the risk of MCI and dementia.
c. Blood pressure: It is important to keep the systolic blood pressure under control…the better the control, the lower the risk of dementia [8].
d. Food: The MIND (The Mediterranean–DASH Intervention for Neurodegenerative Delay) diet, a hybrid of the Mediterranean diet and the DASH (Dietary Approaches to Stop Hypertension) diet, and a controlled calorie-restricted diet, showed no difference in cognition scores. Consumption of flavonols may be associated with reduced dementia risk [10], and mild alcohol drinking may be protective, though heavy drinking is detrimental [11].
This means sensible eating and moderation of addictions are key, as we already know.
e. Control of hearing loss: This improves cognition and reduces dementia risk, but only in those at risk for dementia [12].
We know that diagnosing and treating hearing loss is important for the individual and those around them. This study reinforces that.
Question 3: Is there any new data for mindfulness, social connections, etc.?
“Good social connections (i.e., living with others, weekly community group engagement, interacting weekly with family and friends, and never feeling lonely) are associated with slower cognitive decline.” [13] The negative effect of poor social health on cognition may be partly related to depression [14].
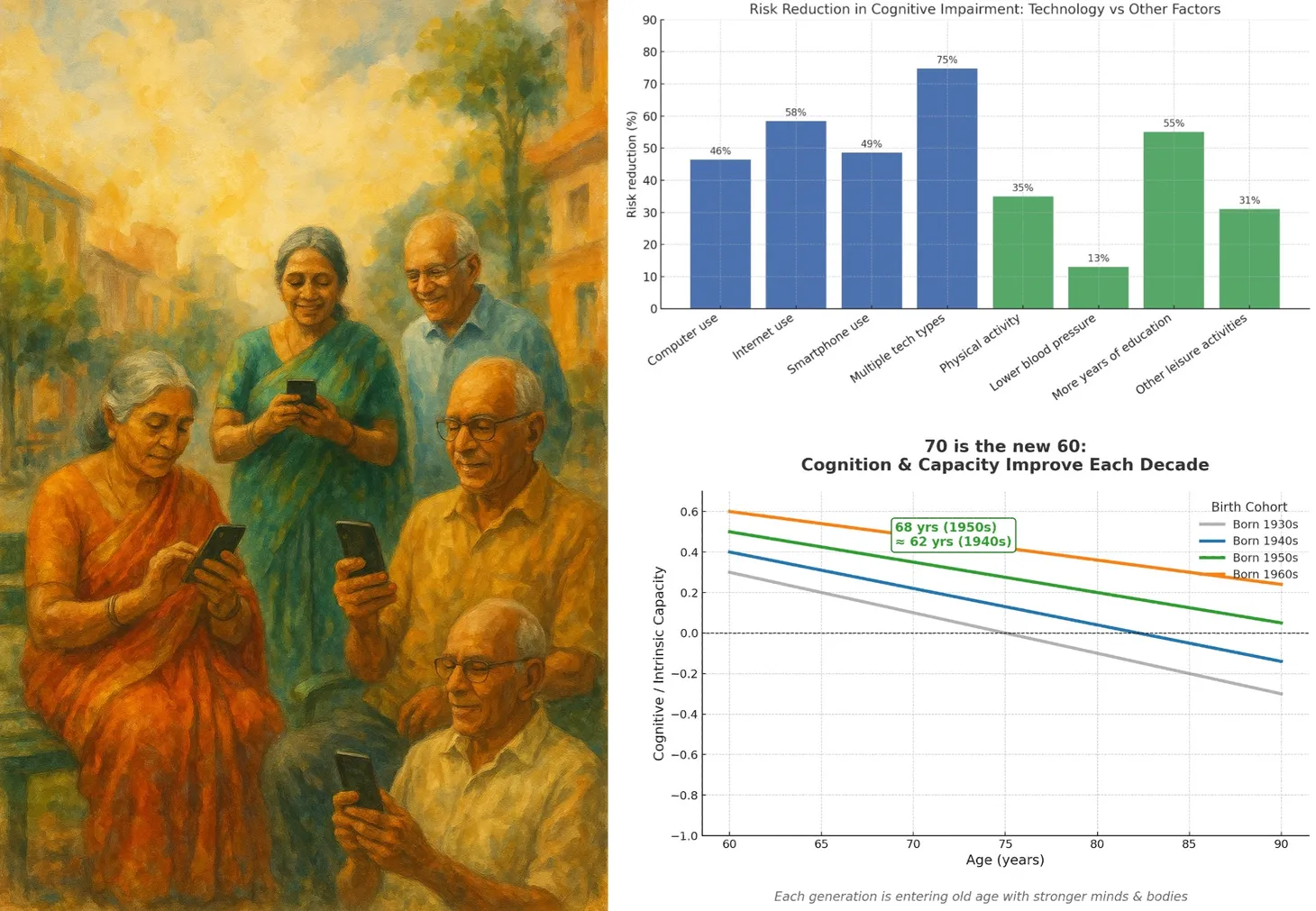
Mindfulness does not seem to work [15], though online internet usage is interestingly associated with reduced risk of dementia [16]. The question to ask then is whether the widespread use of WhatsApp and similar social media tools helps reduce MCI as we age?
Question 4: Can MCI or AD be treated with medicines?
New anti-amyloid monoclonal antibodies have shown promise but have side effects. Aducanumab was fast-tracked by FDA but then withdrawn recently. Lecanemab, a new drug, has been approved and shows promise for men with AD. Time will reveal the effectiveness and benefits of newer therapies [17].

What does this mean for you and I?
Genetic or blood testing for MCI or AD may be premature if you have no signs or symptoms of cognitive impairment because there isn’t much you can do with a positive test. If you want to test though, the current standard of care is a standard cognition test (language, memory, etc.) with a neuropsychologist. However, this may change as the field progresses and I will keep you updated.
Preventing MCI and AD is based on lifestyle factors (sensible eating, physical activity, adequate sleep, not smoking), controlling high blood pressure, diabetes, reducing cardiovascular risk (statins, aspirin, if indicated), and maintaining social connections and increasing cognitive reserve by reading and engaging in activities that stimulate the mind.
In the future, there may be treatment options available for MCI and AD, and I’ll write about them as they emerge.
Footnotes
1 Serrano-Pozo A et al. APOE and Alzheimer's disease: advances in genetics, pathophysiology, and therapeutic approaches. Lancet Neurol. 2021 Jan;20(1):68-80. doi: 10.1016/S1474-4422(20)30412-9.
2 Régy M et al. The role of dementia in the association between APOE4 and all-cause mortality: pooled analyses of two population-based cohort studies. Lancet Healthy Longev. 2024 Jun;5(6):e422-e430. doi: 10.1016/S2666-7568(24)00066-7.
3 Ashton NJ et al. Diagnostic Accuracy of a Plasma Phosphorylated Tau 217 Immunoassay for Alzheimer Disease Pathology. JAMA Neurol. 2024 Mar 1;81(3):255-263. doi: 10.1001/jamaneurol.2023.5319.
4 Oveisgharan S et al. The time course of motor and cognitive decline in older adults and their associations with brain pathologies: a multicohort study. Lancet Healthy Longev. 2024 May;5(5):e336-e345. doi: 10.1016/S2666-7568(24)00033-3. Epub 2024 Apr 3.
5 https://www.newyorkfed.org/medialibrary/media/research/staff_reports/sr1106.pdf?sc_lang=en
6 Veronese N et al. Physical activity and exercise for the prevention and management of mild cognitive impairment and dementia: a collaborative international guideline. Eur Geriatr Med. 2023 Oct;14(5):925-952. doi: 10.1007/s41999-023-00858-y.
7 Jin Y et al. Cardiometabolic multimorbidity, lifestyle behaviours, and cognitive function: a multicohort study. Lancet Healthy Longev. 2023 Jun;4(6):e265-e273. doi: 10.1016/S2666-7568(23)00054-5.
8 Li S et al. Systolic Blood Pressure Time in Target Range and Cognitive Outcomes: Insights From the SPRINT MIND Trial. Hypertension. 2023 Aug;80(8):1628-1636. doi: 10.1161/HYPERTENSIONAHA.122.20711.
9 Barnes LL et a. Trial of the MIND Diet for Prevention of Cognitive Decline in Older Persons. N Engl J Med. 2023 Aug 17;389(7):602-611. doi: 10.1056/NEJMoa2302368. Epub 2023 Jul 18.
10 Holland TM et al. Association of Dietary Intake of Flavonols With Changes in Global Cognition and Several Cognitive Abilities. Neurology. 2023 Feb 14;100(7):e694-e702. doi: 10.1212/WNL.0000000000201541.
11 Jeon KH et al. Changes in Alcohol Consumption and Risk of Dementia in a Nationwide Cohort in South Korea. JAMA Netw Open. 2023 Feb 1;6(2):e2254771. doi: 10.1001/jamanetworkopen.2022.
12 Lin FR et al. Hearing intervention versus health education control to reduce cognitive decline in older adults with hearing loss in the USA (ACHIEVE): a multicentre, randomised controlled trial. Lancet. 2023 Sep 2;402(10404):786-797. doi: 10.1016/S0140-6736(23)01406-X.
13 Samtani S et al. Associations between social connections and cognition: a global collaborative individual participant data meta-analysis. Lancet Healthy Longev. 2022 Nov;3(11):e740-e753. doi: 10.1016/S2666-7568(22)00199-4.
14 Stafford J et al. Social health and subsequent cognitive functioning in people aged 50 years and older: examining the mediating roles of depressive symptoms and inflammatory biomarkers in two European longitudinal studies. Lancet Healthy Longev. 2024 May;5(5):e356-e369. doi: 10.1016/S2666-7568(24)00046-1.
15 Lenze EJ et al. Effects of Mindfulness Training and Exercise on Cognitive Function in Older Adults: A Randomized Clinical Trial. JAMA. 2022 Dec 13;328(22):2218-2229. doi: 10.1001/jama.2022.21680.
16 Cho G et al. Internet usage and the prospective risk of dementia: A population-based cohort study. J Am Geriatr Soc. 2023 Aug;71(8):2419-2429. doi: 10.1111/jgs.18394.
Kim AY et al. Alzheimer's disease and its treatment-yesterday, today, and tomorrow. Front Pharmacol. 2024 May 24;15:1399121. doi: 10.3389/fphar.2024.1399121
Atmasvasth Newsletter
Join the newsletter to receive the latest updates in your inbox.


{kind=link}