The Coronary Calcium Score Test - A Useful Test, But...
The CAC test is helpful but should be used judiciously and preferably on a doctor's recommendation
Text
One of the vagaries of modern medicine and life is that while people get over-tested for cardiac conditions, those who would benefit from testing often fall through the cracks and land up with sudden cardiac death or major cardiac events that affect their subsequent healthspan and lifespan.
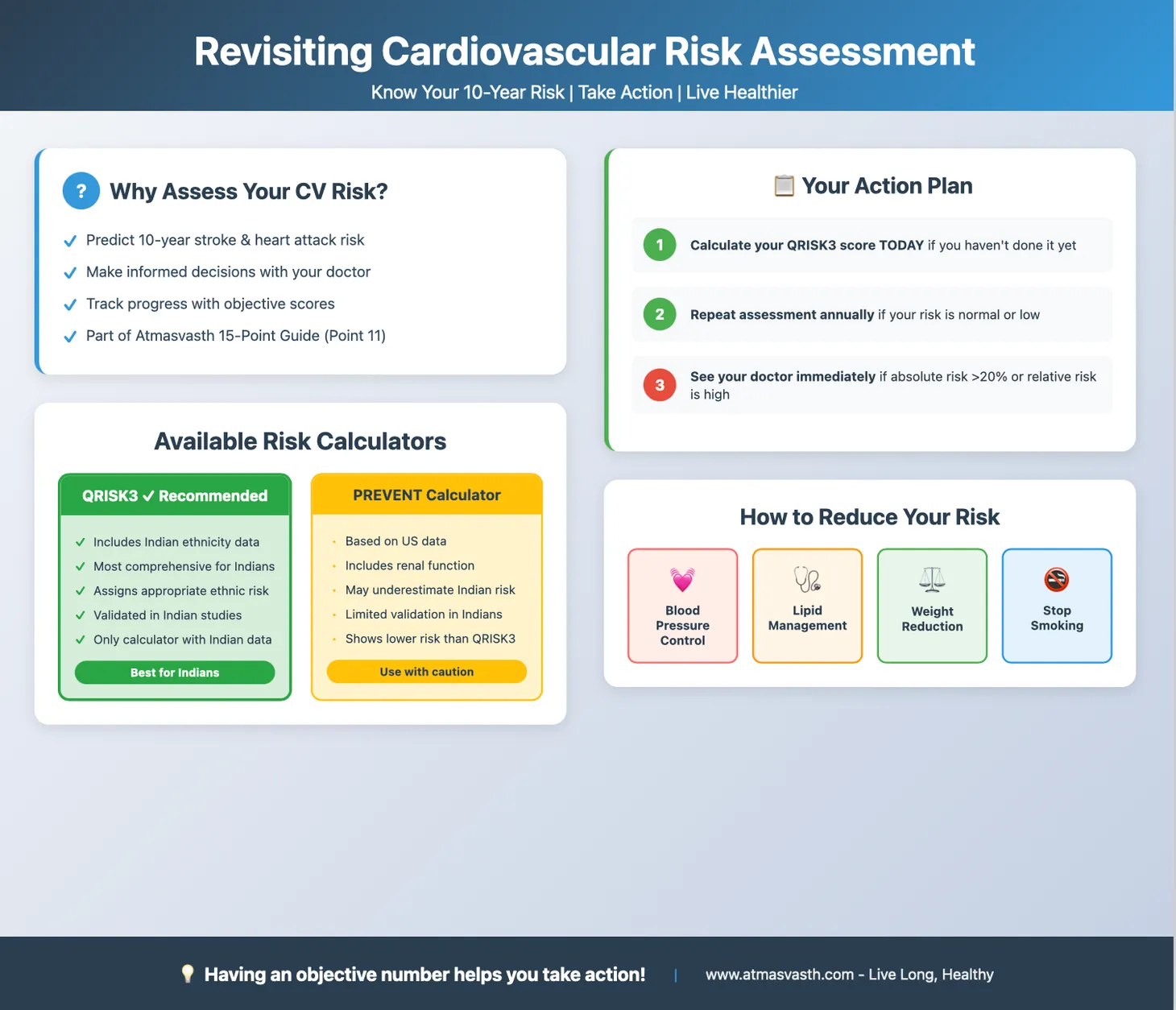
Hence, a focus on cardiovascular risk assessment at regular intervals with QRISK3 and LE8 helps you know if you are at a higher risk than normal of developing cardiac events in the future or not, with the hope that you can and will initiate steps to reduce that risk. Risk reduction involves the following
1. Appropriate physical activity
2. Lipid lowering agents (LLAs) like statins
3. Aspirin
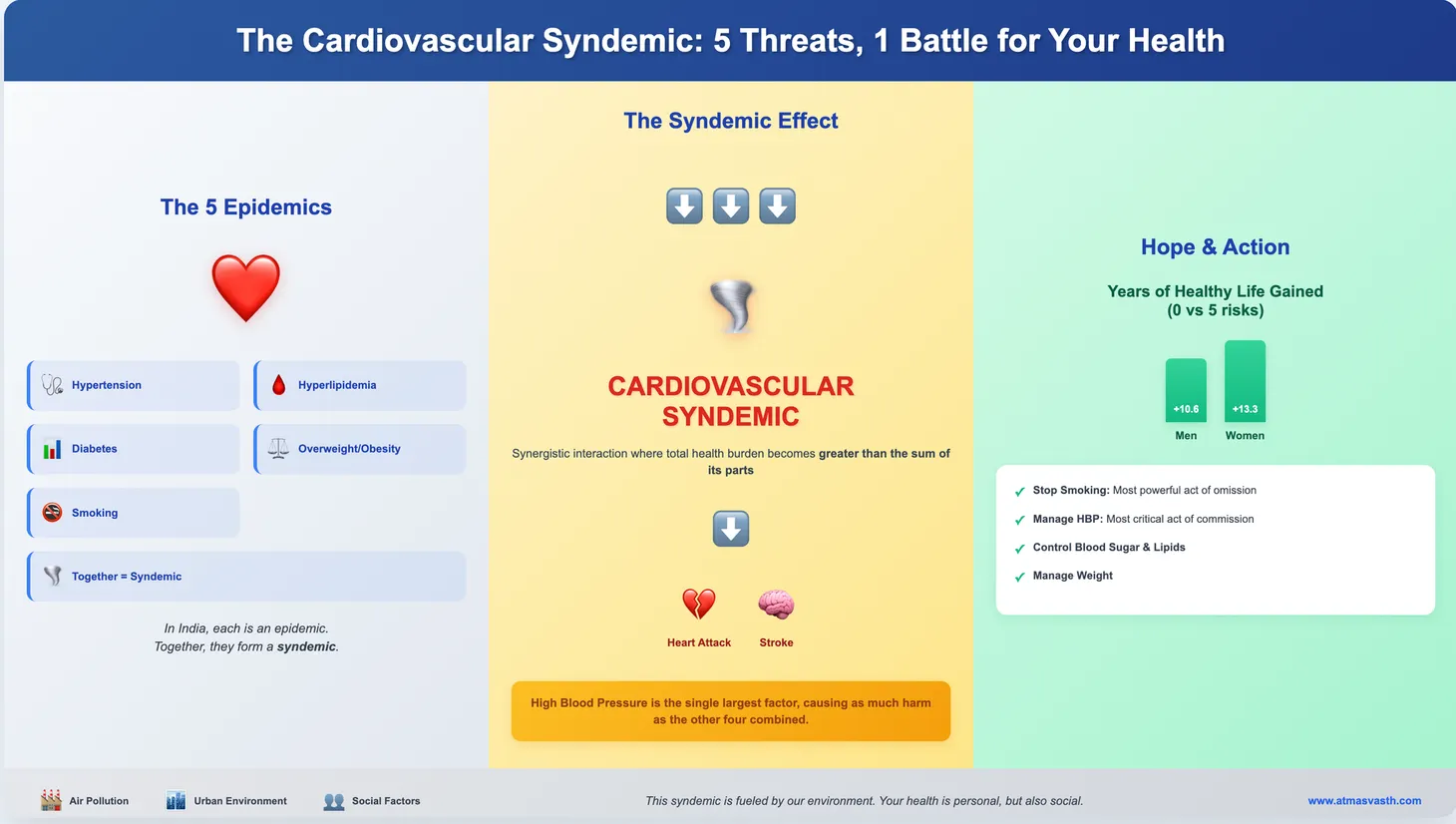
5. Controlling high blood pressure
6. Controlling diabetes
7. Not smoking
While points 1 and 4 seem obvious, many people start with physical activity and sensible eating only when there has been a scare in the family or with themselves. Most people glide through life hoping that nothing much is likely to come in their way of eating whatever they want while staying sedate at home and at work. Point 7 is obvious and thankfully fewer and fewer people are smoking these days, but if you are, just stop. Points 5 and 6 are obvious, but provided these conditions are picked up by testing.
LLAs make a difference when the CV risk is high. When the risk is low or intermediate, they are of uncertain usefulness and like all drugs, not without side-effects, however minimal or small they may be. You must question every pill, Ayurvedic or homeopathic or modern medicine related, that you put inside our body.
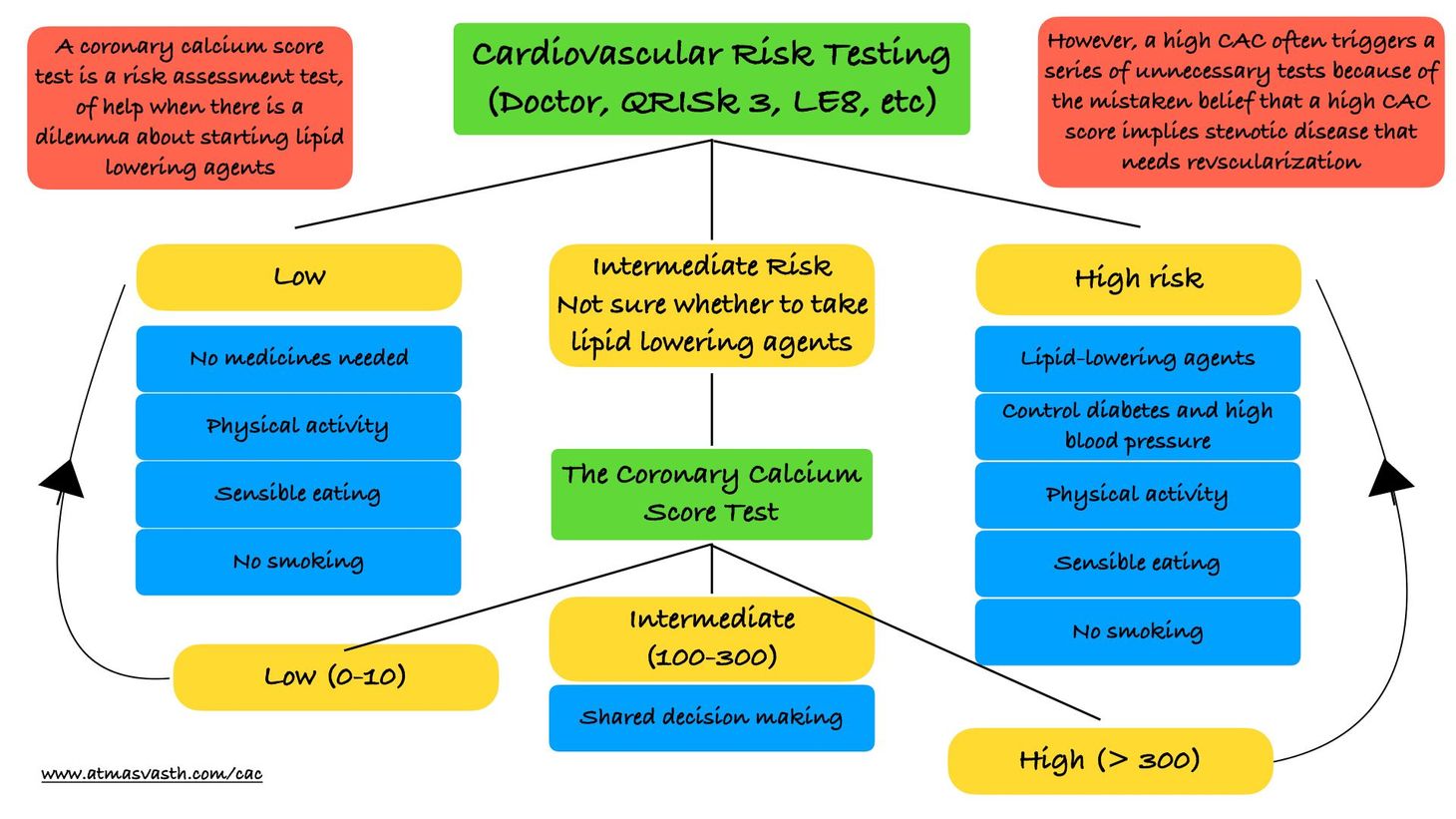
One test that has the potential to change our risk status is the “coronary artery calcium score (CAC)” test. It helps adjust your CV risk and can help you and your doctors decide whether adding LLAs or aspirin will be of help.
Audio
Text (contd)
The CAC test is done in a CT scanner. It takes seconds to perform while the interpretation takes another minute or so.
A CAC score of 0 implies there is no or minimal atherosclerotic disease and the chance of a coronary event in the future is low.
If the CAC score is above 300 or 400 then it implies a higher risk of a cardiac event in the near and medium term future, which would then push you into taking LLAs and/or aspirin depending on the extent of the CAC score and other risk factors.
If you however have intermediate risk on QRISK3 or similar testing, a CAC of 0 can help you decide to not take LLAs and to wait a few years.
However, the CAC test is not universally used for a variety of reasons. It is expensive compared to blood tests and clinical assessment. Many critics also mention the radiation involved, but that is negligible and not relevant. The other problem is that a high CAC score is often handled wrongly by people, who interpret it as the presence of “blocks” and then immediately get themselves or their patients tested with stress echocardiograms or coronary angiograms and if blocks are found, land up with stents or bypasses, even if they are asymptomatic. I have seen this happen so often that my heart sinks when a friend or a relative or a doctor gets a CAC score and then goes berserk if the score is high, instead of understanding that this is just a risk assessor to tell you whether to take LLAs or not.
It is not the fault of the test, but the downstream issues cause unnecessary panic and further testing. Asymptomatic people (and I am using the word “people” not “patients”) do not need further testing with a high CAC score, and even in symptomatic patients with suspected disease but a low pre-test probability based on risk assessment, deferred testing is fine, as a recent analysis of the PROMISE trial has shown [1]. In fact, even patients with chronic stable disease with blocks don’t need bypasses or stents (acute events are different) and hence testing for blocks itself becomes pointless, especially in asymptomatic people, irrespective of the high CAC score, as the ISCHEMIA trial has shown [2].
One of the criticisms of the use of LLAs in primary prevention of coronary artery disease (i.e. in asymptomatic people) is that the number of people needed to be on LLAs to prevent one heart attack is quite high and does not justify putting 80 people on LLAs to prevent 1 person from getting a heart attack, especially if your initial risk is low. The higher your CV risk, the more likely that the LLAs will be of use in preventing a future cardiac event.
One area where there is no argument for the use of LLAs and aspirin is in secondary prevention, i.e. preventing another event in those who have already had a cardiac event or stroke. The data in these patients is very strong that LLAs and aspirin (along with physical activity and sensible eating and control of high blood pressure and diabetes) prevent or reduce future events.
An intriguing paper by Mathew Budoff and colleagues [3] published recently shows that those with a CAC of 300 or higher are equivalent to those in the secondary prevention category. So, the argument goes, that if there is no controversy in instituting aggressive secondary preventive measures, then there should be no controversy treating people with a high CAC as if they are patients who need secondary prevention and hence starting LLAs, a strategy that an accompany editorial strongly supports [4].
There is just one problem and that is the lack of a randomized controlled trial that shows that a strategy incorporating the use of CAC compared to a non-CAC based strategy improves overall and cardiovascular survival.
So what does this mean for you and I? If you have a high CV risk on routine testing (QRISK3, etc), then you should consider taking LLAs to control the serum LDL levels preferably bringing them to below 70 mg/dl, with the guidance of a doctor. If you are at low risk, then no drugs are needed. In both settings, physical activity, improved cardiorespiratory fitness and sensible eating with no smoking are a given.
If you are at intermediate risk, and if you don’t want to start LLAs, then a CAC test may help you decide one way or another. If the CAC is 0 or less than 10, you may not need the drugs. If the CAC is 300 or more, then it may be a good idea to start LLAs. If the CAC is between 10 and 300, you are still faced with a plus/minus choice, which would have to be sorted out based on your specific situation, with your doctor.
It is best to get a CAC test done on the advice of your doctor rather than doing it as part of a health check-up, just because you can afford it or the package throws it in free.
If you do get a CAC test done, and if your score is high, please, please don’t panic. Do NOT get any further testing done if you are asymptomatic, because it will just send you spiraling down a path of more and more testing, ending likely with a stent or bypass, whether you need it or not.
Footnotes
1. Udelson JE et al. Deferred Testing in Stable Outpatients With Suspected Coronary Artery Disease: A Prespecified Secondary Analysis of the PRECISE Randomized Clinical Trial. JAMA Cardiol. 2023 Aug 23:e232614.
2. Maron DJ et al. Initial Invasive or Conservative Strategy for Stable Coronary Disease. N Engl J Med. 2020 Apr 9;382(15):1395-1407.
3. Budoff MJ et al. When Does a Calcium Score Equate to Secondary Prevention?: Insights From the Multinational CONFIRM Registry. JACC Cardiovasc Imaging. 2023 Sep;16(9):1181-1189.
4. Blumenthal RS, Leucker TM. Disruptive Innovation in CVD Primary Prevention: Assessing the Equivalency for Secondary Prevention Strategies. JACC Cardiovasc Imaging. 2023 Sep;16(9):1190-1192.
Atmasvasth Newsletter
Join the newsletter to receive the latest updates in your inbox.

{kind=link}